Invented by Anne Goubier, Beatriz Goyenechea Corzo, Josephine Salimu, Kevin Moulder, Pascal Merchiers, Mark Brown, Sergio Quezada, James Geoghegan, Bianka Prinz, University College London, Cancer Research Technology Ltd, Tusk Therapeutics Ltd, Adimab LLC
Autoimmune diseases, such as rheumatoid arthritis, multiple sclerosis, and inflammatory bowel disease, occur when the immune system mistakenly attacks healthy cells and tissues. Tregs, which express high levels of CD25, are responsible for maintaining immune tolerance and preventing excessive immune responses. By targeting CD25, anti-CD25 antibody agents can selectively deplete or inhibit the function of Tregs, thereby modulating the immune response and potentially treating autoimmune diseases.
Cancer, another major indication for anti-CD25 antibody agents, is characterized by uncontrolled cell growth and evasion of the immune system. Tregs play a role in suppressing anti-tumor immune responses, allowing cancer cells to proliferate unchecked. By targeting CD25 on Tregs, anti-CD25 antibody agents can disrupt the immunosuppressive environment created by these cells, enhancing the anti-tumor immune response and potentially improving the efficacy of cancer treatments.
The market for anti-CD25 antibody agents is driven by the growing understanding of the role of Tregs in autoimmune diseases and cancer. Additionally, the increasing prevalence of these diseases globally is fueling the demand for effective therapies. According to the World Health Organization, autoimmune diseases affect around 5-10% of the global population, while cancer is one of the leading causes of death worldwide.
Several anti-CD25 antibody agents are currently in development or have already received regulatory approval. Daclizumab, a monoclonal antibody targeting CD25, was approved by the U.S. Food and Drug Administration (FDA) for the treatment of relapsing forms of multiple sclerosis. However, it was later withdrawn from the market due to safety concerns. Other anti-CD25 antibody agents, such as basiliximab and otelixizumab, have shown promising results in clinical trials for various indications.
The market for anti-CD25 antibody agents is highly competitive, with several pharmaceutical companies actively engaged in research and development. Companies such as Novartis, Roche, and Bristol Myers Squibb are investing in the development of novel anti-CD25 antibody agents to address the unmet medical needs in autoimmune diseases and cancer.
However, challenges such as high development costs, stringent regulatory requirements, and potential side effects need to be overcome for the successful commercialization of these agents. Additionally, the availability of alternative therapies and the emergence of new treatment modalities, such as gene therapy and cell-based therapies, may pose a threat to the market growth of anti-CD25 antibody agents.
In conclusion, the market for anti-CD25 antibody agents is witnessing significant growth due to the increasing prevalence of autoimmune diseases and cancer. These agents hold great promise in modulating the immune response and improving patient outcomes. However, further research and development efforts are needed to address the challenges and unlock the full potential of anti-CD25 antibody agents in the treatment of these diseases.


The University College London, Cancer Research Technology Ltd, Tusk Therapeutics Ltd, Adimab LLC invention works as follows
The present disclosure contains antibody sequences that are found in antibodies which bind human CD25. The present disclosure, in particular, provides sequences of antihuman CD25 antibodies that do not block CD25 binding to IL-2, or IL-2 Signalling. These sequences of antibodies and antigen-binding parts thereof can be used to create pharmaceutical compositions and treatment methods, including cancer treatments.


Background for Anti-CD25 antibody agents
Cancer immunotherapy is the use of an individual’s immune system in order to treat or prevent cancer. Immunotherapies take advantage of the fact that cancerous cells have molecules that are subtly different on their surfaces and can be detected. Cancer antigens are molecules that can be proteins or carbohydrates. Immunotherapy involves stimulating the immune system to attack tumour cells by using these antigens. Malignant tumours and solid tumours can escape immune surveillance through various mechanisms, both internal to the tumour cells as well as mediated by components in the tumour microenvironment. Infiltration of tumours by regulatory T-cells (Tregs or Tregs), and, specifically, a balance between effector T-cells (Teffs) versus the Tregs, are amongst these factors. A low ratio of Treg to Teff has been suggested as a critical factor (Smyth, M. et al. 2014).
Since their discovery, Tregs are critical for mediating immune homeostasis as well as promoting peripheral tolerance and its establishment. In the context of cancer, their role becomes more complex. Tregs can promote tumour growth as cancer cells produce both tumour and self-associated antigens. Infiltration of Tregs into established tumours is one of the major obstacles to anti-tumour treatment and effective antitumour responses. The suppression mechanisms used by Tregs may contribute to the failure or limitation of current treatments, especially immunotherapies that depend on the induction or enhancement of anti-tumour response (Onishi H. et al.; 2012).
It has been shown that Treg cells are involved in the progression and establishment of tumors, and their absence delays tumor progression in murine models (Elpek and al. 2007; Golgher and al. 2002; Jones and al. 2002; Onizuka and al. 1999; Shimizu and al. 1999). In humans, low ratios of T effector (Teff), compared to Treg, and high Treg infiltration are associated with poor outcomes for multiple cancers. (Shang et. al., 2015.) In contrast, both in humans and mice, a higher Teff/Treg ratio is associated to better immunotherapy responses (Hodi, et. al. 2008; Quezada, 2006). The depletion and treatment of tumour Tregs can be complex. Results of clinical and preclinical studies have been inconsistent. This is mainly due to the inability to identify a specific target for Treg.
CD25 is a potential molecular target for the depletion Tregs. CD25 is also known as interleukin-2 receptor alpha-chain (IL-2R)? CD25, also known as the interleukin-2 high-affinity receptor alpha chain (IL-2R? ), is constitutively induced at high levels on Treg cells. It is absent or only expressed at low levels on T effectors and thus is a promising target to deplete Tregs. The IL-2/CD25 interaction was the subject of many studies in murine model systems, with the majority of these involving PC61, a rat-anti-murine CD25-antibody (Setiady Y et. al., 2010). This antibody’s CD25 binding activity and functional properties were compared with a panel of monoclonal antigens generated by other authors (Lowenthal J.W et. al., 1985. ; Moreau J.-L. et. al. ; Volk H D et al., 1989; Dantal J et al., 1991,). In the original studies, PC61 was shown to have prophylactic, but not therapeutic, activity. However, in a more recent study, it was found that an Fc-optimized version of this anti CD25 antibody depleted intra-tumoral Tregs and offered significant therapeutic benefit for several murine tumor models (Vargas et. al., 2017).
Available anti CD25 antibody such as PC61 blocks or inhibits the binding of IL-2 with CD25. This is true of many anti-mouse CD25 antibodies and of most antibodies disclosed as anti-human CD25 antibodies; see, for example, WO2004/045512 WO2006/108670 WO1993/011238, WO1990/007861 WO2017/174331. Daclizumab and Basiliximab, for example, are anti-human CD25 antibody that inhibits the binding of IL-2 with CD25. They were developed to reduce activation T-effector cell (Queen et al., 1989 and Bielekova, 2013). “Basiliximab, a chimeric human-mouse CD25 antibody that is currently approved for graft against host disease and Daclizumab, a humanized CD25 antibodies approved for multiple sclerosis
A few anti-CD25 antibody clones still allow the binding IL-2 to CD25. These include clone MA251(anti-human CD25), clone clone 7G7B6 (7G7B6) (antihuman CD25). non-blocking antibodies). While it has been claimed that Inolimomab/BT536 does not block binding of IL-2 with CD25, it does block signalling via CD25. 7D4 has been used extensively to detect CD25 positive cells when PC61, or antibodies with similar binding properties have been present or after treatment (Onizuka A et. al. 1999). Few documents describe the functional properties of 7D4 IgM antibodies, either alone or in comparison to PC61 (Kohm et. al. 2006; Hallett et. al. 2008; Fecci p et. al. 2006; McNeill a et. al. 2007; SetiadyY et. al. 2010; Couper K and al. 2007, for example). In fact, the prior art doesn’t teach how to modify or adapt the 7D4 isotype, or any other structural feature, to create an improved antibody that can be used for cancer therapy. “The ability of 7D4 IgM or any engineered anti-human CD25 that has CD25 binding characteristics similar to those of the 7D4 mouse CD25 has not been evaluated in depth with regard to optimized Treg cell depletion.
As discussed above, the infiltration by Treg cells into tumors and a low ratio between effector Teff to Treg can result in a poor clinical outcome. CD25 was identified as a marker for Treg cells and may be an attractive target for therapeutic antibodies that aim to deplete Treg. CD25 is an alpha subunit for the receptor of IL-2, and IL-2 plays a major role in Teff responses. Anti-CD25 antibody that has been tested in clinical trials, while depleting Treg cell numbers also blocks IL-2 signalling through CD25 (specifically a CD25/CD122/CD132 compound). The inventors of the present invention have found that a blockade in IL-2 signalling is limiting Teff responses. They also discovered that an anti CD25 antibody which does not block IL2 signalling, can deplete Treg cell numbers while still allowing IL-2 stimulation to Teff cells.
There is a need for improved anti CD25 antibodies. These should be those that don’t block CD25 from binding to IL-2, or IL-2 signalling. They also must deplete Tregs in tumors and can be used as a treatment for cancer.
The present invention provides anti-CD25 Antibody agents. In certain embodiments, anti-CD25 antibody agents are antibodies or antigen binding fragments that bind specifically to CD25 and particularly human CD25 without blocking interleukin 2(IL-2) or signaling via CD25. They also deplete Tregs in tumors. The anti-CD25 Antibody agents allow at least half of IL-2 to be signaled in response to IL-2 bind to CD25 compared with the level of signaling without the anti-CD25 Antibody agent. Anti-CD25 Antibody agents are therefore referred as non-blocking anti-CD25 Antibody agents or anti-IL-2 blocking anti CD25 Antibody agent.
In some embodiments, anti-CD25 antibodies or antigen-binding fractions bind CD25 but do not block the binding of IL-2 or the signalling of IL-2 through CD25. In some embodiments the anti-CD25 antibody agents or antigen-binding fragments bind CD25 without blocking the binding of IL-2 to CD25 or signalling of IL-2 via CD25. The anti-CD25 antibody is characterized by structural features that allow binding CD25 while not blocking the binding of IL-2 or its signalling.


It was surprising to find that anti-CD25 antibody that does not block IL-2 IL-2 signaling via CD25 but depletes Tregs has a strong anti-tumour impact. In particular, they have a stronger antitumour effect that anti CD25 antibodies which deplete Tregs and block IL-2 signals. The antibodies increased both the CD4+ and CD8+ ratios of Teff/Treg. The depletion and preservation of IL-2 signalling in Teff cells while reducing tumor-infiltrating T-reg cells is a therapeutic strategy that can be used to treat cancer either alone or with other anticancer agents.
Those in the know, however, can appreciate that the teachings of this disclosure are not restricted by a specific mechanism of action for the antibodies provided or antigen-binding fractions thereof. The relevant structural and/or function features of the antibodies provided are described in this document and speak for themselves.
In some embodiments, anti-CD25 Antibody agents are characterized by features that are related to binding to a particular epitope on human CD25 extracellular region, or that make them more suitable for pharmaceutical use and/or manufacture.
The provided technologies are useful for medicine, such as the anti-CD25 Antibody agents (e.g. the provided antibodies, or antigen binding fragments thereof), the compositions that include them, and/or the uses of them. Some embodiments of the provided technologies can be used in cancer treatment and/or prevention.
In some embodiments the anti-CD25 Antibody agents are represented by antibodies with the sequence aCD25-686. These antibodies may also include antibodies that contain the aCD25-686-HCDR3 sequence, which is the variable heavy chain complementarity-determining region 3; or, in other embodiments, antibodies that have both the aCD25-686 HCDR1 or HCDR2 amino acid sequences. The anti-CD25 Antibody Agents described here, such as aCD25-686, also include their variants, including the affinity-matured variants, aCD25-686m1, aCD25-686m2, aCD25-686m3, aCD25-686m4, and aCD25-686m5.
In one embodiment there is an anti-CD25 Antibody agent that contains the HCDR1, HCDR2 & HCDR3 amino acids of aCD25-686. In another embodiment, an anti-CD25 Antibody agent is provided that contains the HCDR1, LCDR1, LCDR2, and LCDR3 sequences of aCD25-686. In a different embodiment, an anti-CD25 Antibody agent is provided that contains the variable heavy amino acids of aCD25-686. In another embodiment, an anti-CD25 Antibody agent is provided that contains the variable heavy and light amino acid sequences from aCD25-686 or a variant thereof. “Equivalent anti-CD25 Antibody Agents are also contemplated based on affinity matured variants of aCD25-686m1, aCD25-686m2, aCD25-686m3, aCD25-686m4, and aCD25-686m5.
In some embodiments, an anti-CD25 Antibody agent is provided that competes with aCD25-686 (or antigen-binding fraction or derivative or variation thereof, including affinity-matured variants) in binding to the human CD25 extracellular region.
In some embodiments, anti-CD25 Antibody agents (e.g. The provided antibodies, antigen-binding fractions thereof (including variants and derivatives, such as affinity maturated variants), or antigen binding fragments thereof bind to human CD25 at a Kd of less than 10?7M. In the range of 10?8 or even 109 or 1010 or 1011 or 1012 or even 1013. In certain embodiments, the anti-CD25 Antibody agents (e.g. The provided antibodies, antigen-binding fractions thereof (including variants and derivatives, such as affinity maturated variants), bind to CD25 in humans with a Kd of 10?7-10?10 or 10?7-10?9.
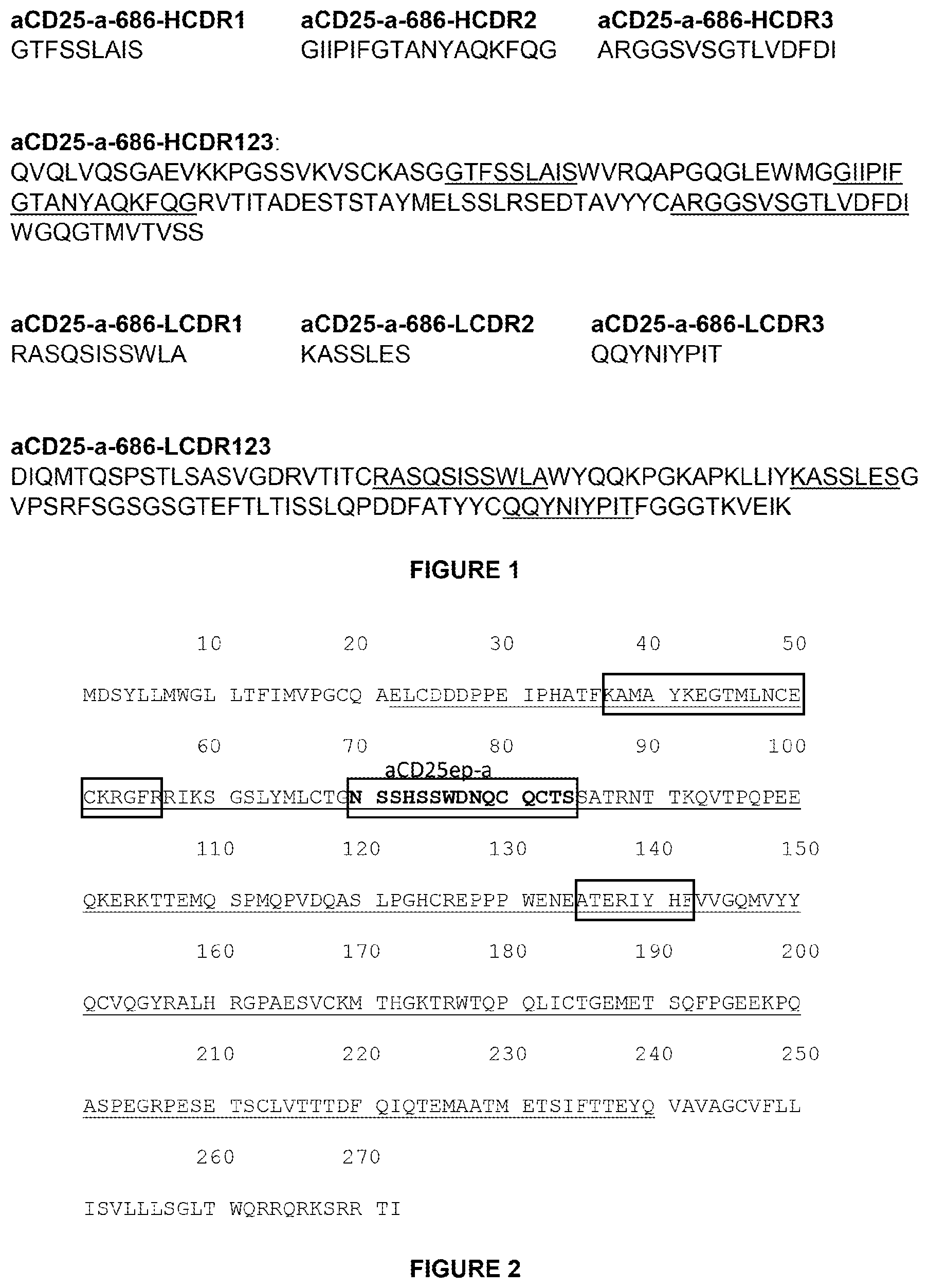
In some embodiments, anti-CD25 antibody agents (e.g. the provided antibodies, antigen binding fragments or derivatives or derivatives of the antibodies), bind to a CD25 epitope that is bound by aCD25-686. In certain embodiments, the anti-CD25 Antibody agents may bind human CD25’s extracellular domain. In certain embodiments, anti-CD25 antibody agents may bind to a CD25 epitope (e.g. when assessed by one or more assays described herein, or other assays known in the field), and in particular, one identified as aCD25ep a (SEQ NO: 23). In certain embodiments, the anti-CD25 Antibody Agents provided antibodies or antigen-binding fractions according to the invention bind specifically to the epitopes designated aCD25ep a (SEQID NO: 23), aCD25ep b (SEQID NO: 24), or aCD25ep c (SEQID NO: 25). The anti-CD25 Antibody Agents antibodies, or antigen-binding fragments, according to the present invention, bind specifically to epitopes such as aCD25ep a (SEQ ID NO: 23), aCD25ep b (SEQ ID NO: 24), or aCD25ep c (SEQID No: 25)(see FIG. The anti-CD25 Antibody Agents antibodies or antigen binding fragments provided in one embodiment of the invention bind specifically to aCD25epb and/or aCD25epc.
In some embodiments the provided anti-CD25 Antibody Agents (e.g. to an extracellular epitope on human or non-human primate, such as Cynomolgus Monkey CD25), may bind with a Kd-value in the range of 10-7 M or lower, for example, in the ranges 10-8, 10-9, 10-10, 10-11, 10-12, or 10-13. In some embodiments, the anti-CD25 Antibody agents (e.g. The provided antibodies, antigen-binding fractions thereof (including variants and derivatives, such as affinity maturated variants), bind to CD25 in humans with a Kd of 10?7-10?10 or 10?7-10?9.


The present disclosure also provides a method that can be used to identify and/or characterization of particularly useful anti CD25 Antibody agents (e.g. anti-CD25 antibody or antigen binding fragments thereof), as described in this document (e.g. anti-CD25 antibody or antigen binding fragments thereof characterized with certain structural and/or function features, such a specific binding to CD25 human (e.g. an extracellular epitope of it), inclusion of CDR sequences as described in this document In some embodiments the anti-CD25 antibody agents described herein can be characterized by multiple features. In certain embodiments, the anti-CD25 antibody agents described herein can be one or more of the antibodies.


Click here to view the patent on Google Patents.







